Enlarged Prostate (BPH)
Enlarged Prostate (BPH)
BPH is an enlarged prostate. The prostate goes through two main growth cycles during a man’s life. The first occurs early in puberty, when the prostate doubles in size. The second phase of growth starts around age 25 and goes on for most of the rest of a man's life. BPH most often occurs during this second growth phase.
As the prostate enlarges, it presses against the urethra. The bladder wall becomes thicker. One day, the bladder may weaken and lose the ability to empty fully, leaving some urine in the bladder. Narrowing of the urethra and urinary retention – being unable to empty the bladder fully – cause many of the problems of BPH.
BPH is benign. This means it is not cancer. It does not cause or lead to cancer. However, BPH and cancer can happen at the same time.
BPH is common. About half of all men between ages 51 and 60 have BPH. Up to 90% of men over age 80 have it.

Diagram of Normal and Enlarged Prostate Enlarge
What is the Prostate
The prostate is part of the male reproductive system. It is about the size of a walnut and weighs about an ounce. The prostate is found below the bladder and in front of the rectum. It goes all the way around a tube called the urethra, which carries urine from the bladder out through the penis.
The prostate’s main job is to make fluid for semen. During ejaculation, sperm made in the testicles moves to the urethra. At the same time, fluid from the prostate and the seminal vesicles also moves into the urethra. This mixture – semen – goes through the urethra and out through the penis.
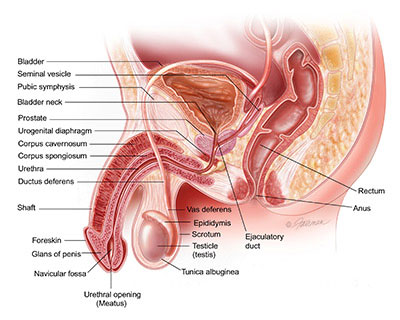
Diagram of the Male Reproductive System Enlarge
Symptoms
When the prostate is enlarged, it can bother or block the bladder. Needing to urinate often is a common symptom of BPH. This might be every 1 to 2 hours, mainly at night.
Other symptoms include:
- Feeling that the bladder is full, even right after urinating
- Feeling that urinating "can't wait"
- A weak flow of urine
- Needing to stop and start urinating several times
- Trouble starting to urinate
- Trouble starting to urinate
- Needing to push or strain to urinate
If BPH becomes severe, you might not be able to urinate at all. This is an emergency that must be treated right away.
How Can BPH Affect Your Life?
In most men, BPH gets worse with age. It can lead to bladder damage and infection. It can cause blood in the urine and cause kidney damage.
Causes
The causes of BPH are not well-understood. Some researchers believe that factors related to aging and the testicles may cause BPH. This is because BPH does not develop in men whose testicles were removed before puberty.
Throughout their lives, men produce both testosterone, a male hormone, and small amounts of estrogen, a female hormone. As men age, the amount of active testosterone in the blood lowers, leaving a higher share of estrogen. Studies have suggested that BPH may happen because the higher share of estrogen in the prostate adds to the activity of substances that start prostate cells to grow.
Another theory points to dihydrotestosterone (DHT), a male hormone that plays a role in prostate development and growth. Some research has shown that, even when testosterone levels in the blood start to fall, high levels of DHT still build up in the prostate. This may push prostate cells to continue to grow. Scientists have noted that men who do not produce DHT do not develop BPH.
Who is at Risk for BPH?
Aging and a family history of BPH increase a man’s risk for BPH. Obesity, lack of staying active, and erectile dysfunction can also increase risk.
Can BPH be Prevented?
There is no sure way to stop BPH, but losing weight and eating a healthy diet that involves fruits and vegetables may help. This may relate to having too much body fat, may increase hormone levels and other factors in the blood, and stimulate the growth of prostate cells. Staying active also helps control weight and hormone levels.
Diagnosis
See your doctor if you have symptoms that might be BPH. See your doctor right away if you have blood in your urine, pain or burning when you urinate, or if you cannot urinate.
Your doctor can diagnose BPH based on
- Personal or family history
- A physical exam
- Medical tests
The American Urological Association (AUA) has built a BPH Symptom Score Index. It’s a series of questions about how often urinary symptoms happen. The score rates BPH from mild to severe. Take the test and talk with your doctor about your results.
Your doctor will review your Symptom Score and take a medical history. You will also have a physical exam that involves a digital rectal exam (DRE). Your doctor may also want you to have some or all of these tests:
- Cystoscopy to look at the urethra or bladder with a scope
- Post-void residual volume to measure urine left in the bladder after urinating
- PSA blood test to screen for prostate cancer
- Ultrasound of the prostate
- Urinalysis (urine test)
- Uroflowmetry to measure how fast urine flows
- Urodynamic pressure to test pressure in the bladder during urinating
- Urinary blood test to screen for bladder cancer
PSA Blood Test
Prostate-specific antigen (PSA) is a protein that is made only by the prostate. When the prostate is healthy, very little PSA is found in the blood.
The PSA blood test measures the level of PSA in the blood. The test can be done in a lab, hospital, or doctor's office. No special preparation is needed. The PSA test should be done before the doctor does a DRE. You should not ejaculate for 2 days before a PSA test. That’s because ejaculation can raise the PSA level for 24 to 48 hours.
A low PSA is better for prostate health. A rapid rise in PSA may be a sign that something is wrong. BPH is one possible cause of a high PSA level. Inflammation of the prostate, or prostatitis, is another common cause of a high PSA level.
Digital Rectal Exam
The DRE is done with the man bending over or lying curled on his side. The doctor puts a lubricated, gloved finger into the rectum to feel the shape and thickness of the prostate. The DRE can help your doctor find prostate problems.

Diagram of Digital Rectal Exam of the Prostate Enlarge
Treatment
There are many options for treating BPH. You and your doctor will decide together which treatment is right for you. Mild cases may need no treatment at all. In some cases, minimally invasive procedures (surgery without anesthesia) are good choices. And sometimes a combination of treatments works best.
The main types of treatments for BPH are:
- Active Surveillance
- Prescription Drugs
- Less Invasive Surgery
- More Invasive Surgery
Active Surveillance
Often, BPH will only require active surveillance. If you and your doctor choose this treatment option, your BPH will be closely watched but not actively treated. This means that BPH is monitored with regular visits to your urologist. A yearly exam is common. Your health care provider will look for worse or new issues before suggesting anything else. Diet and exercise are often recommended as a way to prevent or manage your symptoms.
Active surveillance is best for men with mild to moderate symptoms. It is also an option for men who are not bothered by the effects of BPH. If your symptoms get worse, or if new symptoms appear, your doctor may suggest that you begin active treatment.
Prescription Drugs
Alpha Blockers
Alpha blockers relax the muscles of the prostate and bladder. They improve urine flow, reduce blockage of the urethra and reduce BPH symptoms. They do not reduce the size of the prostate. Men with moderate to severe BPH and men who are bothered by their symptoms are good candidates. Alpha blockers are not a good choice for men who are about to have cataract surgery.
These prescription drugs are pills taken by mouth. Alpha-blocking drugs include alfuzosin, doxazosin, silodosin, tamsulosin and terazosin.
Side effects may include dizziness, lightheadedness, fatigue and trouble ejaculating. One benefit of alpha blockers is they start to work right away.
5-Alpha Reducatase Inhibitors
5-alpha reductase inhibitors block the production of DHT, a male hormone that can build up in the prostate and may cause prostate growth. They shrink the prostate, increase urine flow and reduce the risk of BPH complications. They also make it less likely that you will need surgery. These drugs may be best for men with very large prostate glands.
These prescription drugs are pills taken by mouth and include dutasteride and finasteride. They may take many months to become fully effective.
Side effects include erectile dysfunction and reduced libido (sex drive). You must keep taking the pills to prevent symptoms from coming back.
Combined Therapy
With combined therapy, an alpha blocker and a 5-alpha reductase inhibitor are used together. Men with larger prostates are good candidates for this treatment.
Alpha blockers and 5-alpha reductase inhibiters may work better together than either drug does alone. They improve symptoms and prevent BPH from getting worse.
Possible drug combinations include:
- Finasteride and doxazosin
- Dutasteride and tamsulosin, a combination that is available in a single tablet
- Alpha blockers and antimuscarinics
A urologist may add antimuscarinics for patients with overactive bladder symptoms. Overactive bladder is when the bladder muscles squeeze uncontrollably. It leads to the frequent and urgent need to pass urine. It can lead to incontinence (leaking). Antimuscarinics relax the bladder muscles.
Side effects may happen with each drug. By taking two drugs, you may have more side effects than if you were taking just one. Some side effects in patients on combination therapy were dizziness, erectile dysfunction, weakness or lack of energy and a drop in blood pressure when moving from sitting or lying down to standing.
Phytotherapies
Phytotherapies are herbal treatments. They are not prescribed by a doctor, but are sometimes a form of "self-treatment."
Men buy them over the counter as dietary supplements. One popular herb is saw palmetto. Several important studies show they do not work. Also, the quality and purity of supplements vary. Doctors do not currently recommend herbal treatments for BPH.
Less Invasive Surgery
Minimally invasive or less invasive surgeries require only tiny cuts or no cuts to the body. Good candidates include men who have taken BPH medication that did not work or men with the following symptoms:
- Weak stream of urine
- Straining to pass urine
- Urinary tract obstruction, bladder stones and/or blood in your urine
- Incomplete emptying
- Bleeding from the prostate
They can often be done as an outpatient, without a stay in the hospital. Recovery time is usually quicker. They can offer relief from symptoms, including urine control problems. On the other hand, they do not reduce your risk for another surgery.
Side effects for having certain types of minimally invasive surgery is the increased risk you will need to have another surgery or need to go back on medications. Other temporary side effects may include:
- Blood in the urine
- Burning when you pass urine
- Needing to pass urine more often
- Sudden urges to pass urine
- Urinary Tract Infection
- Less often, erectile dysfunction or retrograde ejaculation (semen flowing backward into the bladder instead of out of the penis)
Choosing the right type of surgery for you may depend on the size of your prostate, your overall health and your personal choice. Some types of surgeries ARE NOT recommended to include prostate artery embolization (PAE) and transurethral needle ablation (TUNA). Yet, there are many types of less invasive surgeries your doctor may suggest.
Types of Less Invasive Surgeries
Prostatic Urethral Lift (PUL)
PUL uses a needle to place tiny implants in the prostate. These implants lift and compresses the enlarged prostate so that it no longer blocks the urethra. PUL may be done with either local or general anesthesia.
PUL uses no cutting or heat to destroy or remove prostate tissue. It takes less than an hour and you can usually go home the same day. Most men see symptom improvement within about two weeks. Flow rates tend to be better with TURP; however, men who undergo PUL tend to be very pleased with the less invasive procedure.
Some men may have pain or burning when passing urine, blood in the urine or a strong urge to pass urine. These side effects usually go away within two to four weeks. Men may have fewer sexual side effects after PUL than after other types of prostate surgery.
Men with many medical problems may be good candidates. Men for whom surgery is high-risk may also be good candidates. Many men with enlarged prostates and urinary symptoms may be good candidates for PUL. Men who have PUL can still have other treatment if they need it, including MRI, TURP, etc. If you are allergic to nickel, titanium, or stainless steel, talk to your doctor before getting PUL. Current studies have evaluated seven years of treatment with PUL and future studies may help to determine long term durability.
Water Vapor Thermal Therapy
This treatment uses water vapor (steam) to destroy prostate cells squeezing the urethra.
Inside a handheld device, sterile water is heated to just above the boiling point, when it turns into steam. A precise dose of thermal energy from the steam is then injected into the prostate with a small needle. The release of this thermal energy causes rapid cell death. The body’s natural healing response then breaks down and removes the dead tissue, causing the prostate to shrink.
The treatment is done in the doctor’s office with local anesthesia or after you have taken a pill for pain. You may have blood in your urine and need to use a catheter for a few days. Painful or frequent urination should go away within about two to three weeks. Sexual side effects, such as erectile dysfunction, are unlikely.
Studies currently suggest that symptom improvement lasts for at least five years. It is not currently known whether the treatment continues to work long-term (beyond the five-year point) or whether patients eventually need to have additional treatment.
Men may be good candidates if they do not want to take medication for BPH or if they have tried medication and found it did not work. Unlike other less invasive therapies, this therapy can treat men who have a middle lobe of the prostate. Men who prefer not to have surgery or want to avoid sexual side effects may also be good candidates.
Transurethral Microwave Therapy (TUMT)
TUMT uses microwaves to destroy prostate tissue. The urologist threads a catheter through the urethra to the prostate. A device called an antenna sends microwaves through the catheter to heat selected portions of the prostate. The heat destroys excess prostate tissue. A cooling system protects the urinary tract from heat damage during the procedure.
TUMT does not require general anesthesia. The surgeon numbs the skin and gives you a pain pill. TUMT only takes an hour. It may relieve bladder obstruction. There is little blood loss or fluid absorption. You can usually go home the same day. TUMT poses a low risk of side effects, such as urinary tract infections, urinary incontinence and scarring in the urethra. Some men have symptoms to include frequent or intense urges to pass urine and a burning feeling when passing urine. Newer therapies have largely replaced this practice.
Men with too many medical problems for invasive surgery may be good candidates for TUMT. Men with weak hearts may be good candidates because there is minimal blood loss. So are men who want to avoid anesthesia.
Catheterization
Catheterization uses a tube called a catheter in the bladder to drain urine. Catheters can be placed through the urethra or via a small puncture in the bladder above the pubic bone. This option is helpful for men with bladder control problems and a blocked prostate. Still, catheters' benefits are temporary.
There are two types of catheters. The catheter may be "clean," which means it is placed and removed every six to eight hours. Or it may be "indwelling," which means it is left in the bladder for a short or long time.
Side effects of using catheters may be infection. When a catheter is in place for a long time bacteria can stick to the catheter surface. This makes it hard for the immune system or antibiotics to work. Using a catheter for a few years increases risk for bladder cancer and can destroy the tissue of the penis. This is probably due to the long-term irritation caused by the catheter sitting in the bladder or at the meatus (urine opening at the tip of the penis). The risk of infection and cancer is lower with “clean intermittent catheterization” than with an “indwelling” catheter.
Good candidates for using catheters include men who are waiting for medication to work or waiting for surgery. Catheters are also used during treatment for an infection. They may be a good choice for men who have many medical problems and for men toward the end of their lives, when surgery is not advised.
More Invasive Surgery
In severe cases of BPH, or when other options fail, more invasive surgery is recommended. More invasive surgery is best if you:
- Are unable to pass urine
- Have kidney damage
- Have frequent urinary tract infections
- Have a lot of bleeding
- Have stones in the bladder
There are several options. The best option will depend on your health, your doctor’s expertise and your personal choice.
Types of More Invasive Surgeries
Options below appear in order of least invasive to most invasive.
Transurethral Incision of the Prostate (TUIP)
TUIP may be used if you have a smaller prostate but still have major blockage of the urethra. Instead of cutting and removing tissue, TUIP widens the urethra. The surgeon uses a laser beam or an electrical current to make small cuts in the bladder neck, where the urethra joins the bladder, and in the prostate. This reduces the pressure of the prostate on the urethra and makes urination easier. A catheter is left in your bladder for one to three days after surgery. The hospital stay is one to three days.
TUIP may improve the ability to pass urine. It may ease symptoms. Temporary urine retention, urinary tract infection, dry orgasm, incontinence and erectile dysfunction are possible side effects. Some men need additional treatment after TUIP.
Men who have a smaller prostate or do not want a more complete prostate resection but need surgery are good candidates for TUIP. The procedure is less likely to interfere with ejaculation than the more substantial TURP.
Photoselective Vaporization (PVP)
PVP is a very common surgery for BPH. In PVP, the surgeon guides a thin tube (a cystoscope) through the urethra to the prostate. Then the surgeon uses a laser to destroy obstructing prostate tissue and stop bleeding.
PVP is done as an outpatient procedure at the hospital or sometimes in the doctor’s office. Most men can have a PVP without adverse events. There is little bleeding and few side effects. After PVP, you can often stop medical therapy for BPH.
Good candidates for PVP include men with small- to moderate-sized prostates and those with too many medical problems for more-invasive surgery. Men with weak hearts are also good candidates because there is no blood loss. So are men who want to limit anesthesia. Men with a higher risk of bleeding, such as those taking blood-thinning medications, may also be good candidates for PVP.
Transurethral Resection of the Prostate (TURP)
TURP is also a very common surgery for BPH. After anesthesia, the surgeon inserts a thin, tube-like instrument (a resectoscope) through the tip of the penis into the urethra. The resectoscope has a light, valves for irrigating fluid and a thin wire loop. An electrical current is passed along the wire. The surgeon uses the electrified wire to cut away prostate tissue that is blocking the urethra and seal blood vessels. The removed tissue is flushed into the bladder and from there out of the body. You will need to use a catheter for one to two days after the procedure.

Diagram of Transurethral Resection of the Prostate (TURP) Enlarge
This treatment has well known long-term outcomes. Other treatments are generally compared with it. Symptoms generally improve markedly. The effects of treatment last for 15 years or more.
TURP does not remove the entire prostate. No incisions (cuts) are needed. The hospital stay is one to two days or until there is no significant blood in your urine. TURP does require anesthesia. As with any surgery, anesthesia poses a risk.
Side effects of TURP may include retrograde ejaculation, erectile dysfunction, urinary tract infections right after surgery and urinary incontinence. Full recovery takes about four to six weeks.
Men who require surgery because of moderate to severe BPH symptoms may be good candidates for TURP.
Holmium Laser Enucleation of Prostate (HoLEP)
In HoLEP, the surgeon places a thin, tube-like instrument (a resectoscope) through the penis into the urethra. A laser inserted into the resectoscope destroys the excess prostate tissue.
No incisions (cuts) are needed. You may only need to stay one night in the hospital. There is very little bleeding. A catheter is used, but it is usually removed the next day. You may have blood in your urine or frequent or painful urination for a few days. This treatment requires anesthesia. Men having HoLEP have more post-operative stress urinary incontinence compared to the other surgeries, but this improves in about one year. As with any surgery, anesthesia poses a risk.
Men with larger prostates who wish to avoid more-invasive surgery may be good candidates for this treatment. Men with a higher risk of bleeding, such as those taking blood-thinning medications, may also be good candidates for HoLEP.
Thulium Laser Enucleation of the Prostate (ThuLEP)
ThuLEP is similar to HoLEP but uses a different type of laser. As in HoLEP, the surgeon places a thin, tube-like instrument (a resectoscope) through the penis into the urethra. A laser inserted into the resectoscope destroys the excess prostate tissue.
No incisions (cuts) are needed. There is very little bleeding. Recovery is rapid. A catheter may be used, but it is usually removed the next day. You may have blood in your urine or frequent or painful urination for a few days. You may only stay one night in the hospital. But this treatment requires anesthesia. As with any surgery, anesthesia poses a risk.
Men with larger prostates who wish to avoid more-invasive surgery may be good candidates for this treatment. Men with a higher risk of bleeding, such as those taking blood-thinning medications, may also be good candidates for ThuLEP.
Transurethral Vaporation of the Prostate (TUVP)
In TUVP, the surgeon inserts a thin, tube-like instrument (a resectoscope) into the urethra. This instrument has a lens, a light, and a tool that sends out an electrical current to destroy prostate tissue. Heat from the electrical current seals small blood vessels, reducing the risk of bleeding.
There is little bleeding or fluid absorption. You may stay one night in the hospital and you can usually return home without a catheter. This treatment requires anesthesia. As with any surgery, anesthesia poses risks.
Men with larger prostates who wish to avoid more-invasive surgery may be good candidates for TUVP.
Transurethral Water–Jet Ablation (TWJA)
TWJA uses high-pressure water jets to destroy excess prostate tissue. The surgeon first uses ultrasound to precisely map the location of the excess tissue. Then the high-pressure water jets are directed to that area. Following this, the surgeon inserts another instrument to seal small blood vessels to reduce the risk of bleeding. The patient needs to stay in the hospital one night to irrigate the bladder to prevent blood clots. You may need to use a catheter for about 48 hours after the procedure and should be able to go home the next day.
After Treatment
For most men, symptoms of BPH improve after treatment. Infection, bleeding, incontinence, and erectile dysfunction may occur after some treatments. In some cases, scar tissue may form.
What are the Long–Term Side Effects of Treatment?
Side effects vary with the type of treatment you choose. Most side effects are temporary. It may take a while for sexual function to fully return. Most experts agree that if you were able to have an erection shortly before surgery, you will probably be able to do so after surgery. Most men find little or no difference in orgasm. You may have retrograde ejaculation (when semen enters the bladder rather than being sent out through the penis). For most men, side effects lessen with time. Some treatments may cause long-term side effects for some men.
How Can You Prevent a Recurrence of BPH?
Once you have been treated for BPH, taking medication can prevent symptoms from returning or getting worse. Some men may need additional treatment. Some men need repeated treatment to get rid of bothersome symptoms. In older men, it may be possible to control BPH symptoms to the end of life.
Experimental Therapies without Proven Benefit
Prostate Artery Embolization (PAE)
PAE is a new procedure for treating BPH that is still being tested in clinical trials in the United States. Clinical trials are research studies that test how well new treatments work in people.
In PAE, tiny round particles are injected through a catheter into the vessels that supply blood to the prostate. The particles block blood flow to the large blood vessels (arteries) of the prostate. This causes the prostate to shrink.
Because PAE is new and still being tested, little is known for sure about how well it works and what side effects it may cause. At this time, the American Urological Association advises that patients should be treated with PAE only in a clinical (experimental) trial.